The Bottom Line: “Drug-induced immune hemolytic anemia is a rare occurrence that results from drug-induced antibodies. A DAT result is positive in patients with this condition. The progression of the condition is typically gradual, and treatment involves removal of the offending agent.” (Phillips)
The Bottom Line: Though there is a possible connection supported by some case reports and a few retrospective cohort studies, a definitive causation of military occupational exposure to radar with hemolymphatic and other cancers has not been established. However, physicians can still consider hemolymphatic cancer in their differential diagnosis if they know their patient has had occupational exposure to radar.
In their retrospective cohort study of a previously published case series of 47 patients diagnosed with cancer following years of occupational exposure to radiofrequency radiation (RFR), Peleg (2018) found “the consistent association of RFR and highly elevated HL cancer risk in the four groups spread over three countries, operating different RFR equipment types and analyzed by different research protocols, suggests a cause-effect relationship between RFR and HL cancers in military/occupational settings.”
In 2023, Peleg et. al published a second study analyzing data from a new case series of 46 patients diagnosed with cancer that had exposure to radar in a military setting and comparing them with similar groups from other studies, finding “a consistent, statistically significant, and well-documented atypically high HL PF, distinctly higher than expected in the community (Cancer Registry) or computed from unexposed comparison groups.”
The Bottom Line: “Patients with symptoms of heart failure and those with risk factors should be examined for pulmonary rales, jugular venous distention, a third heart sound, and peripheral edema and should have an ECG and chest radiograph” (Badgett)
“Very helpful findings [for detection of heart failure] are radiographic redistribution and jugular venous distention. These findings, when used alone, only help when they are abnormal and so can confirm the presence of increased filling pressure in patients with known severe systolic dysfunction. Among patients referred for consideration of cardiac transplant with a high (73%) prevalence of increased filling pressure, radiographic redistribution indicates an 80% to 90% probability and jugular venous distention, an85% to 100% probability of increased filling pressure. The absence of either finding cannot rule out increased filling pressure. In patients with lesser probabilities of increased filling pressure, such as those without known severe systolic dysfunction, isolated findings may not be useful. Somewhat helpful findings include dyspnea and abnormal vital signs. Radiographic cardiomegaly is somewhat helpful but loses its specificity after the initial detection of increased filling pressure because it can be a permanent finding and not fluctuate with changes in filling pressure. Dependent edema is helpful only when present. Edema is highly specific for increased filling pressure, although it has poor sensitivity.” (Badgett)
(Badgett)
“Patients with heart failure can have decreased exercise tolerance with dyspnea, fatigue, generalized weakness, and fluid retention, with peripheral or abdominal swelling and possibly orthopnea. Patient history and physical examination are useful to evaluate for alternative or reversible causes. Nearly all patients with heart failure have dyspnea on exertion. However, heart failure accounts for only 30 percent of the causes of dyspnea in the primary care setting. The absence of dyspnea on exertion only slightly decreases the probability of systolic heart failure, and the presence of orthopnea or paroxysmal nocturnal dyspnea has a small effect in increasing the probability of heart failure (positive likelihood ratio [LR+] = 2.2 and 2.6).” (King)
The Bottom Line: “Antifungal therapy is recommended for all cases of [catheter-related bloodstream infection] CRBSI due to Candida species, including cases in which clinical manifestations of infection and/or candidemia resolve after catheter withdrawal and before initiation of antifungal therapy” (Mermel)
“Fluconazole administered at a dosage of 400 mg daily for 14 days after the first negative blood culture result is obtained is equivalent to amphotericin B in the treatment of candidemia caused by Candida albicans and azole-susceptible strains [184]. For Candida species with decreased susceptibility to azoles (e.g., C. glabrata and C. krusei), echinocandins (caspofungin administered with a 70-mg intravenous loading dose, followed by 50 mg daily administered intravenously; micafungin at a dosage of 100 mg daily administered intravenously or anidulafungin with a 200-mg intravenous loading dose followed by 100 mg daily administered intravenously) or lipid formulations of amphotericin B (ambisome or amphotericin B lipid complex) administered intravenously at a dosage of 3–5 mg/kg daily are highly effective [185–187]. Conventional amphotericin B therapy is also effective but is associated with more adverse effects.” (Mermel)
“The administration of appropriate antimicrobial treatment more than 12 h after the first positive blood sample for culture is drawn is associated, at least by multivariable analysis, with hospital mortality. This underscores the clinical importance of providing early appropriate treatment to patients with fungal bloodstream infections. Future studies are needed to define the optimal strategy for the empiric treatment of fungal bloodstream infections. Until such data become available, clinicians may consider the use of empiric antifungal therapy in patients at high risk for this infection to avoid delays in treatment.” (Morrell)
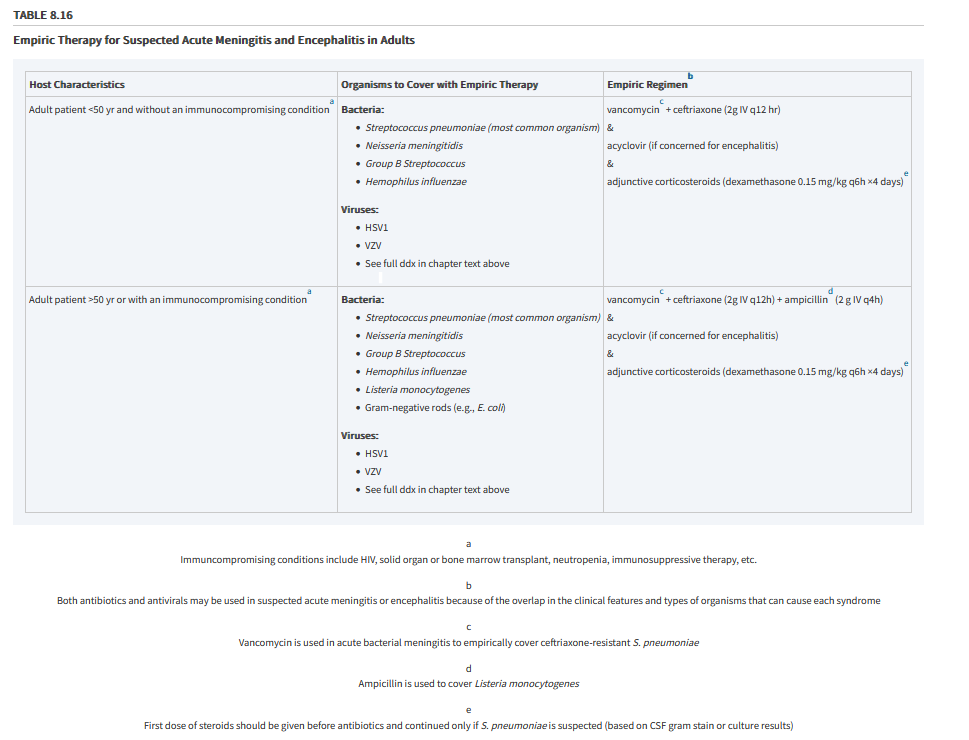
The Bottom Line: “An analysis for different bacteria causing meningitis showed that patients with meningitis due to Streptococcus pneumoniae (S pneumoniae) treated with corticosteroids had a lower death rate (29.9% versus 36.0%.” “Subgroup analyses for causative organisms showed that corticosteroids reduced mortality in Streptococcus pneumoniae (S pneumoniae) meningitis (RR 0.84, 95% CI 0.72 to 0.98.” (Brouwer)
“The National Comprehensive Cancer Network (NCCN), the American College of Chest Physicians (ACCP, and the American Society of Clinical Oncology (ASCO)) have created guidelines for the diagnosis and treatment of lung cancer. They advise the following recommendations:
Patients with a strong clinical suspicion of stage 1 or 2 lung cancer (based on risk factors and radiologic appearance) do not require a biopsy before surgery. A biopsy adds time, costs, and procedural risk and may not be needed for treatment decisions.
A preoperative biopsy may be appropriate if a non-lung cancer diagnosis is strongly suspected that can be diagnosed by core biopsy or fine needle aspiration.
A preoperative biopsy may be appropriate if an intraoperative diagnosis appears difficult or very risky. If a preoperative tissue diagnosis has not been obtained, then an intraoperative diagnosis (ie, wedge resection, needle biopsy) is necessary before lobectomy or pneumonectomy.
Invasive mediastinal imaging is recommended before surgical resection for most patients with clinical stage 1 or 2 lung cancer.
The preferred diagnostic strategy for an individual patient depends on the size and location of the tumor, the presence of mediastinal or distant disease, patient characteristics (such as pulmonary pathology and/or other significant comorbidities), and local experience and expertise.
The least invasive biopsy with the highest yield is preferred as the first diagnostic study.
Anatomic pulmonary resection is preferred for the majority of patients with NSCLC.
Patients suspected of having the metastatic disease should have confirmation from one of the metastatic sites if feasible but should have a biopsy of the primary lung lesion or mediastinal lymph nodes if it is technically difficult or very risky to biopsy a metastatic site.
Patients with metastatic disease should have the histologic subtype established with adequate tissue for molecular testing (including consideration for re-biopsy or plasma biopsy) to enable the best guidance for chemotherapy options.
Decisions about the optimal diagnostic steps for suspected stage 1 to 3 lung cancer should be made by thoracic radiologists, interventional radiologists, interventional pulmonologists, and thoracic surgeons who devote a significant portion of their practice to thoracic oncology.
A joint decision among a radiologist, a pulmonologist, and a medical or radiation oncologist is the desirable approach.
In patients suspected of having small cell lung cancer (SCLC) based on radiographic and clinical findings, it is recommended that a pathologic diagnosis be confirmed by the least invasive method (sputum cytology, thoracentesis, fine needle aspiration (FNA), or transbronchial aspiration, as dictated by the patient’s presentation (Grade 1C).
In patients suspected of having lung cancer who have a solitary extrathoracic site suspicious of metastasis, it is recommended that tissue confirmation of the metastatic site be obtained if an FNA or biopsy of the site is feasible (Grade 1C).
In patients suspected of having lung cancer who have lesions in multiple distant sites suspected of metastases but in whom biopsy of a metastatic site would be technically difficult, it is recommended that diagnosis of the primary lung lesion be obtained by the least invasive method (Grade 1C).
In patients suspected of having lung cancer with a peripheral lung nodule, when tissue diagnosis is required due to the uncertainty of diagnosis or poor surgical candidacy, radial EBUS is recommended as an adjunct imaging modality (Grade 1C). If radial EBUS is thought to be unlikely to achieve a diagnosis, then electromagnetic navigation guidance is recommended if the equipment and the expertise are available (Grade 1C). Remark: If electromagnetic navigation is not available, then percutaneous lung lesion biopsy is recommended.
If specimens obtained initially are not adequate for histologic and molecular characterization, then pursuing a second biopsy is acceptable, given the importance of accurate tumor characterization.
In the case of a small (less than 3 cm), solitary, peripheral lung lesion that is suspicious for lung cancer in a patient who appears to have early-stage disease and is a surgical candidate, the diagnostic dilemma generally centers around whether it is necessary to obtain a biopsy specimen to confirm the diagnosis of cancer before surgical resection is carried out. When the lesion is moderate to highly suspicious for lung cancer, surgical excision performed via thoracoscopy is the most definitive method of establishing a diagnosis and determining treatment. In nodules with an indeterminate likelihood of malignancy, sampling via percutaneous lung lesion biopsy or bronchoscopy with or without guidance technology (radial EBUS or electromagnetic navigation) may be considered.” (Young)
The Bottom Line: “Since the overall accuracy of JAH and other clinical signs [of meningitis] is in poor to fair range, they do not have good performance alone in detection of meningitis. It seems that physicians should not solely rely on a single test or sign, and they should consider a collection of clinical signs and symptoms and history to have a better judgment. A lot of retrospective and prospective studies have shown that diagnosis of meningitis should be made according to the results of physical examination, history and CSF analysis.” (Ala)
In their 2018 prospective study, Ala et al. found that “that diagnostic value of JAH in diagnosis of meningitis in emergency department is higher than other clinical signs such as Kernig, Brudzinski and neck stiffness but the accuracy of all the mentioned signs is in poor to fair range (AUC 60 to 80). JAH had the highest sensitivity (84.4%) and Kernig and Brudzinski had the highest specificity (89.3% and 90.6%, respectively) among the evaluated signs.” (Ala)
(Ala)
This is congruent with the finds of prospective studies by Nakao et al. (2014) and Mofidi et al. (2017), that the Kernig and Brudzinski signs have low sensitivity but high specificity. And that along with Jolt Accentuation, the absence of the clinical signs of meningitis cannot rule out the diagnosis of meningitis.
“Although poorly sensitive, the physical examination findings of Kernig sign, Brudzinski sign, nuchal rigidity, vomiting, and rash were all relatively specific for both pleocytosis and moderate pleocytosis; however, because sensitivity was low for all of these features, LRs suggest that these findings are ultimately unhelpful. For the finding of moderate pleocytosis, however, high specificity resulted in potentially useful, although not diagnostic, LRs for a positive finding of jolt accentuation, Kernig sign, and Brudzinski sign.” (Nakao)
However, the “combination of Jolt accentuation, Kernig’s sign, and Brudzinski’s sign has 100% specificity and PPV and a very high LR+, so we can suppose a high possibility of meningitis for a patient with headache and fever and a positive result of all of 3 tests.” (Mofidi)
The Bottom Line: Visual hallucinations have numerous etiologies. Outside of psychiatric causes, there are a range of etiologies including, but not limited to: neurological, ophthalmic, pharmacological, toxic metabolic, and physiological causes known to manifest visual hallucinations.
“The most common etiologies for visual hallucinations are dementia and delirium, particularly in geriatric patients. Diseases such as Alzheimer’s, Parkinson’s or Lewy bodies disease should be included in differential diagnostics together with retinal degeneration, cerebrovascular accidents, abuse of psychoactive substances or psychiatric diseases. In what concerns CBS, visual deterioration should be evident in most cases and therefore it occurs with greater frequency in elderly patients exhibiting age-related macular degeneration or glaucoma, most hallucinations being visual (even though CBS cases have been described with associated auditive or tactile hallucinations).” (Dupré-Peláez)
The Bottom Line: “Pneumothorax is an extremely rare and dangerous complication of SLE with only 14 previously reported cases.” “In the literature, glucocorticoids have been shown to negatively impact wound healing, which can result in tissue fragility, leading to a pneumothorax. Fourteen (93%) of the 15 patients, including this study’s patient, were being treated with glucocorticoids before the occurrence of the pneumothorax. The high usage of glucocorticoids in cases of pneumothorax in patients with SLE may suggest that treatment with glucocorticoids could be a risk factor. In addition, glucocorticoids have been reported to hinder the recovery from prior pneumothorax, which may explain the high reoccurrence rate (60%) in these 15 patients.” (Kong)
The Bottom Line: “As opposed to [other] modalities, cardiac magnetic resonance (CMR) has excellent contrast resolution that allows for superior soft tissue characterization. The combined evaluation of morphology, composition, and perfusion makes CMR a useful tool in the assessment of cardiac masses”” (Pazos-López)
“Transthoracic 2-dimensional echocardiography is the most common imaging technique used for cardiac mass evaluation, but it is operator dependent, offers poor tissue characterization, and has acoustic window restrictions in a subset of patients. Transesophageal and 3-dimensional echocardiography may overcome some of these limitations. Computed tomography is also useful for the evaluation of tumors and thrombi, although at the expense of radiation exposure.” (Pazos-López)