“A sudden decrease in serum alcohol concentrations can result in alcohol withdrawal syndrome symptoms within 6 to 8 hours, typically peaking at 72 hours and diminishing by 5 to 7 days. These signs and symptoms can be vague, including anxiety, tremors, headache, nausea/vomiting, diaphoresis, or palpitations, which can progress to delirium tremens. If initial alcohol withdrawal syndrome symptoms do not progress to a more severe stage, they will often resolve within 48 hours.” (Gottlieb)
The Bottom Line: “Acute cholecystitis must be differentiated from other diseases that cause right upper quadrant abdominal pain and nausea or vomiting, such as biliary colic and acute cholangitis.” “Acute cholangitis is defined by fever, jaundice, and right upper quadrant pain with the ultrasound revealing dilated intra-hepatic and extrahepatic biliary ducts. Other diagnoses to consider in a patient presenting with symptoms of acute cholecystitis include acute gastritis, peptic ulcer disease, hiatal hernia, acute pancreatitis, acute viral hepatitis, acute appendicitis, and myocardial infarction.” “Acute, complicated cholecystitis is defined as cholecystitis with the presence of either gallbladder necrosis, perforation, pericholecystic abscess, or cholecystoenteric fistula. Patients with these complications are at higher risk for adverse outcomes after cholecystectomy. Even though antibiotic therapy should be initiated at the time of presentation, nonoperative management is not appropriate for these patients because antibiotics will be inadequate in the setting of necrotic tissue or abscess.” (Gallaher)
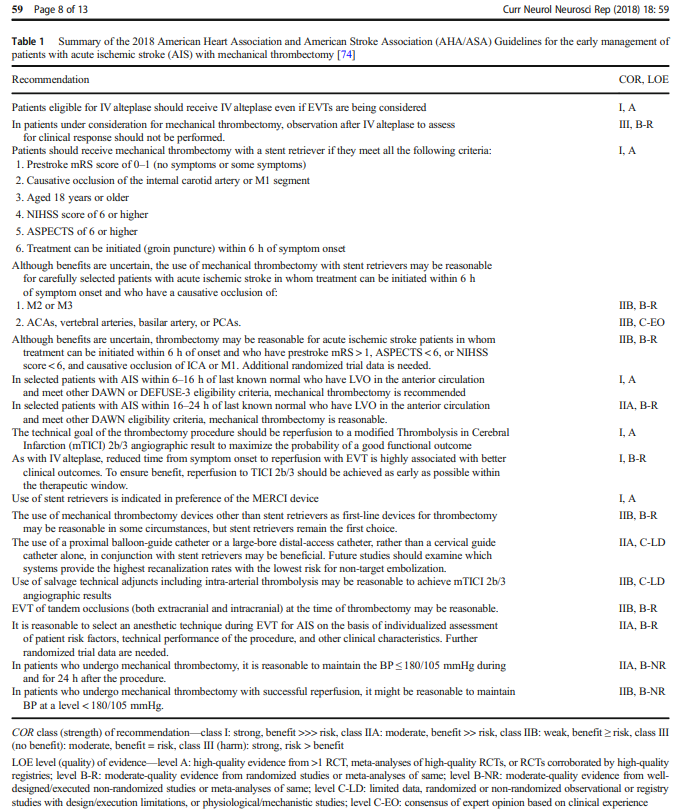
The Bottom Line: “Endovascular therapy (particularly mechanical thrombectomy with stent retriever) is a treatment option to achieve reperfusion in adults with functionally disabling acute ischemic stroke up to 24 hours after stroke onset. Eligibility includes large vessel occlusion on imaging and expected favorable outcomes after reperfusion if ≤ 6 hours after stroke onset or if there is evidence of salvageable brain tissue if 6-24 hours after onset.” (Dynamed)
From the Guidelines for the Early Management of Patients With Acute Ischemic Stroke from the American Heart Association and American Stroke Association (Powers):
“3.7.2. 0 to 6 Hours From Onset
Patients should receive mechanical thrombectomy with a stent retriever if they meet all the following criteria: (1) prestroke mRS score of 0 to 1; (2) causative occlusion of the internal carotid artery or MCA segment 1 (M1); (3) age≥18 years; (4) NIHSS score of≥6; (5) ASPECTS of≥6; and (6) treatment can be initiated (groin puncture) within 6 hours of symptom onset
Direct aspiration thrombectomy as first-pass mechanical thrombectomy is recommended as noninferior to stent retriever for patients who meet all the following criteria: (1) prestroke mRS score of 0 to 1; (2) causative occlusion of the internal carotid artery or M1; (3) age ≥18 years; (4) NIHSS score of ≥6; (5) ASPECTS ≥6; and (6) treatment initiation (groin puncture) within 6 hours of symptom onset.
Although the benefits are uncertain, the use of mechanical thrombectomy with stent retrievers may be reasonable for carefully selected patients with AIS in whom treatment can be initiated (groin puncture) within 6 hours of symptom onset and who have causative occlusion of the MCA segment 2 (M2) or MCA segment 3 (M3) portion of the MCAs.
Although its benefits are uncertain, the use of mechanical thrombectomy with stent retrievers may be reasonable for patients with AIS in whom treatment can be initiated (groin puncture) within 6 hours of symptom onset and who have prestroke mRS score >1, ASPECTS<6, or NIHSS score <6, and causative occlusion of the internal carotid artery (ICA) or proximal MCA (M1)
Although the benefits are uncertain, the use of mechanical thrombectomy with stent retrievers may be reasonable for carefully selected patients with AIS in whom treatment can be initiated (groin puncture) within 6 hours of symptom onset and who have causative occlusion of the anterior cerebral arteries, vertebral arteries, basilar artery, or posterior cerebral arteries.
3.7.3. 6 to 24 Hours From Onset:
In selected patients with AIS within 6 to 16 hours of last known normal who have LVO in the anterior circulation and meet other DAWN or DEFUSE 3 eligibility criteria, mechanical thrombectomy is recommended.
In selected patients with AIS within 16 to 24 hours of last known normal who have LVO in the anterior circulation and meet other DAWN eligibility criteria, mechanical thrombectomy is reasonable”
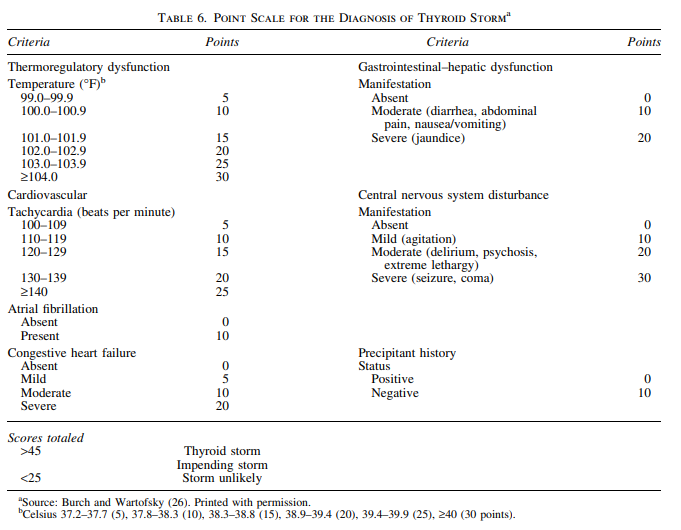
The Bottom Line: “Thyroid storm is diagnosed as a combination of thyroid function studies showing low to undetectable thyroid stimulating hormone (TSH) (<0.01mU/L) with elevated free thyroxine (T4) and/or triiodothyronine (T3), positive thyroid receptor antibody (TRab) (if Graves’ disease is the underlying etiology), and with clinical signs and symptoms of end organ damage. Treatment involves bridging to a euthyroid state prior to total thyroidectomy or radioactive iodine ablation to limit surgical complications such as excessive bleeding from highly vascular hyperthyroid tissue or exacerbation of thyrotoxicosis.” (De Almeida)
“The diagnosis of thyroid storm should be made clinically in a severely thyrotoxic patient with evidence of systemic decompensation. Adjunctive use of a sensitive diagnostic system should be considered. Patients with a Burch– Wartofsky Point Scale (BWPS) of ‡45 or Japanese Thyroid Association ( JTA) categories of thyroid storm 1 (TS1) or thyroid storm 2 (TS2) with evidence of systemic decompensation require aggressive therapy. The decision to use aggressive therapy in patients with a BWPS of 25–44 should be based on clinical judgment.” (Ross)
The Bottom Line: “Antifungal therapy is recommended for all cases of [catheter-related bloodstream infection] CRBSI due to Candida species, including cases in which clinical manifestations of infection and/or candidemia resolve after catheter withdrawal and before initiation of antifungal therapy” (Mermel)
“Fluconazole administered at a dosage of 400 mg daily for 14 days after the first negative blood culture result is obtained is equivalent to amphotericin B in the treatment of candidemia caused by Candida albicans and azole-susceptible strains [184]. For Candida species with decreased susceptibility to azoles (e.g., C. glabrata and C. krusei), echinocandins (caspofungin administered with a 70-mg intravenous loading dose, followed by 50 mg daily administered intravenously; micafungin at a dosage of 100 mg daily administered intravenously or anidulafungin with a 200-mg intravenous loading dose followed by 100 mg daily administered intravenously) or lipid formulations of amphotericin B (ambisome or amphotericin B lipid complex) administered intravenously at a dosage of 3–5 mg/kg daily are highly effective [185–187]. Conventional amphotericin B therapy is also effective but is associated with more adverse effects.” (Mermel)
“The administration of appropriate antimicrobial treatment more than 12 h after the first positive blood sample for culture is drawn is associated, at least by multivariable analysis, with hospital mortality. This underscores the clinical importance of providing early appropriate treatment to patients with fungal bloodstream infections. Future studies are needed to define the optimal strategy for the empiric treatment of fungal bloodstream infections. Until such data become available, clinicians may consider the use of empiric antifungal therapy in patients at high risk for this infection to avoid delays in treatment.” (Morrell)
The Bottom Line: “Treatment of diabetic foot ulcer should be systematic for an optimal outcome. The most important point is to identify if there is any evidence of ongoing infection, by obtaining a history of chills, fever, looking for the presence of purulence or presence of at least two signs of inflammation that includes, pain, warmth, erythema or induration of the ulcer. It should is noteworthy that even in the presence of severe diabetic foot infection, there can be minimal systemic signs of infection.” “The next step is to decide if the patient’s ulcer can is manageable in the outpatient setting or inpatient setting. Need for parenteral antibiotics, concern for noncompliance, inability to care for the wound, ability to offload pressure, are few points to be considered for hospitalization. Both categories of patients should have treatment with antibiotics.” (Oliver)
The Bottom Line: “Managing AF in patients with systolic HF or HF and reduced ejection fraction (HFrEF) remains a therapeutic challenge with several important considerations. Although pharmacological therapies aimed to reduce the risk of stroke and to treat HF may improve patient outcomes, no specific pharmacological approach using rate or rhythm control strategies to manage AF have shown superiority for HF hospitalization or survival. Recently, randomized controlled trials and meta-analyses have demonstrated the effectiveness of catheter ablation (CA) in improving hard end points such as survival, HF hospitalizations, functional capacity, and quality of life (QOL), with acceptable safety, in patients with AF and HFrEF.” (Gopinathannair)
The Bottom Line: “Cystic fibrosis is an autosomal recessive inherited defect in the cystic fibrosis transmembrane conductance regulator (CFTR) gene resulting in abnormal regulation of salt and water movement across the membranes. In the liver this leads to focal biliary fibrosis resulting in progressive portal hypertension and end-stage liver disease in some individuals. This can be asymptomatic, but may lead to splenomegaly and hypersplenism, development of varices and variceal bleeding, and ascites.” (Palaniappan)
Diagnosis of CFLD should be made when at least two of the following variables are present (Debray 2011): • abnormal physical examination: a palpable liver edge more than 2 cm below the bottom edge of the rib cage on the mid-clavicular line and a prominent left lobe palpable in the epigastrium, confirmed by ultrasound; • abnormal liver function tests: an increase in transaminases (aspartate aminotransferase (AST) and alanine aminotransferase (ALT)) and gamma-glutamyl transpeptidase (GGT) levels above the upper normal limits on at least three consecutive occasions over 12 months, after other causes of liver disease; • ultrasonographic evidence of liver involvement (an increased parenchymal echogenicity, irregular margins, nodularity) or PHT (splenomegaly, increased think ness of lesser omentum, spontaneous spleno-renal anastomosis, large collateral veins, ascites) or biliary abnormalities (bile duct dilatation); • a liver biopsy may be indicated if there is diagnostic doubt (Palaniappan)
The Bottom Line: “In patients with acute myocardial infarction and anemia, a liberal transfusion strategy did not significantly reduce the risk of recurrent myocardial infarction or death at 30 days. However, potential harms of a restrictive transfusion strategy cannot be excluded.” “Our results show that in patients with acute myocardial infarction and anemia, a liberal transfusion strategy did not significantly reduce the risk of recurrent myocardial infarction or death at 30 days. Trial end points suggest some benefit of a liberal strategy over a restrictive strategy, but additional studies would be needed to confirm that conclusion.” (Carson)
The Bottom Line: “In this secondary analysis of electronic health data from the high temporal resolution MIMIC III database, metoprolol was the most commonly used pharmacologic agent for control of atrial fibrillation with RVR in the ICU. Metoprolol had a lower ‘failure’ rate as compared to amiodarone and was more likely than diltiazem to achieve rate control at 4-hours. There was no significant difference in hospital mortality based on choice of initial agent.” (Moskowitz)