The Bottom Line: “Idiopathic inflammatory myopathy (IIM) includes dermatomyositis (DM), polymyositis (PM), overlap myositis (OM), sporadic inclusion body myositis (IBM) and necrotising autoimmune myopathy (NAM), also known as immune-mediated necrotising myopathy. DM, OM and NAM all present similarly, with proximal weakness and elevated creatine kinase (CK) level. By contrast, IBM preferentially involves the long finger flexors and quadriceps, and presents with a normal or only mildly elevated CK. Developments in serological testing and imaging are shifting the diagnostic paradigm away from a reliance on histopathology.” (Ashton)
“There is some debate as to whether PM exists as a discrete entity, or is an ill-defined condition encompassing connective tissue disease (CTD) associated myositis, or OM, and the previously poorly recognised NAM” (Ashton)
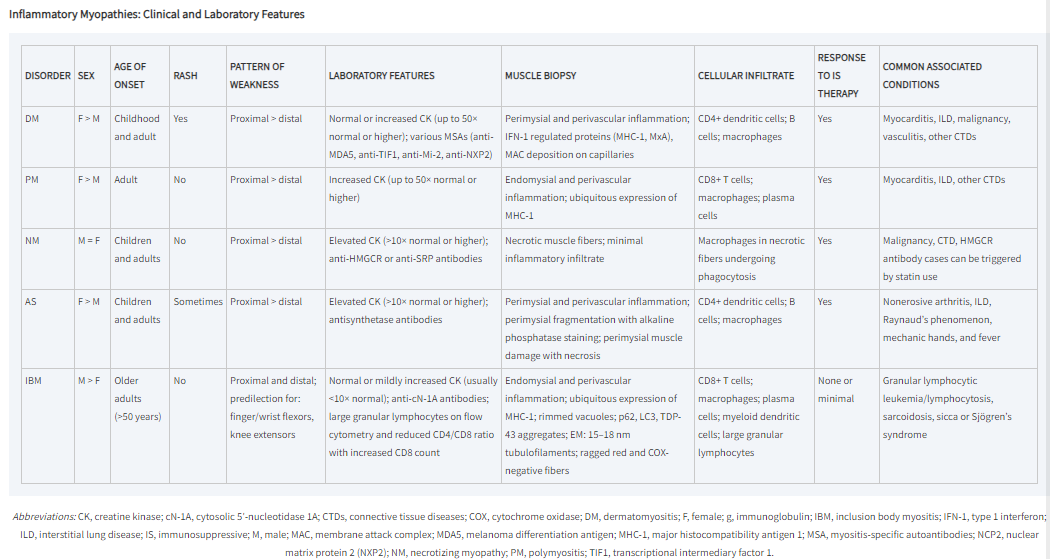
“Epidemiologic studies suggest that the incidence of IM grouped together is >4 cases per 100,000 with prevalence in the range of 14–32 per 100,000. Defining the actual incidence and prevalence of the individual myositides is limited, however, by the different diagnostic criteria employed in various epidemiologic studies, increasing recognition of AS, and frequent misdiagnosis of IBM and IMNM. Idiopathic PM without signs of an overlap syndrome is quite rare, while DM, IBM, and IMNM occur in roughly similar frequencies. DM can occur in children (juvenile DM), while IBM always occurs in adults and is the most common cause of myopathy in those aged >50. DM, PM, and AS are more common in women, while IBM is more common in men.” (Greenberg & Amato)
Continue reading